How crisis centers connect inbound services, coordination responsibilities, and outcome pathways across the broader crisis care continuum.
Crisis centers often serve as the coordination point between inbound demand and downstream support. This visual shows how crisis lines, local warm lines, diversion pathways, third-party reports, and community programs can connect through the crisis center to outcome pathways such as de-escalation, mobile crisis dispatch, stabilization, respite referral, and post-crisis wraparound.
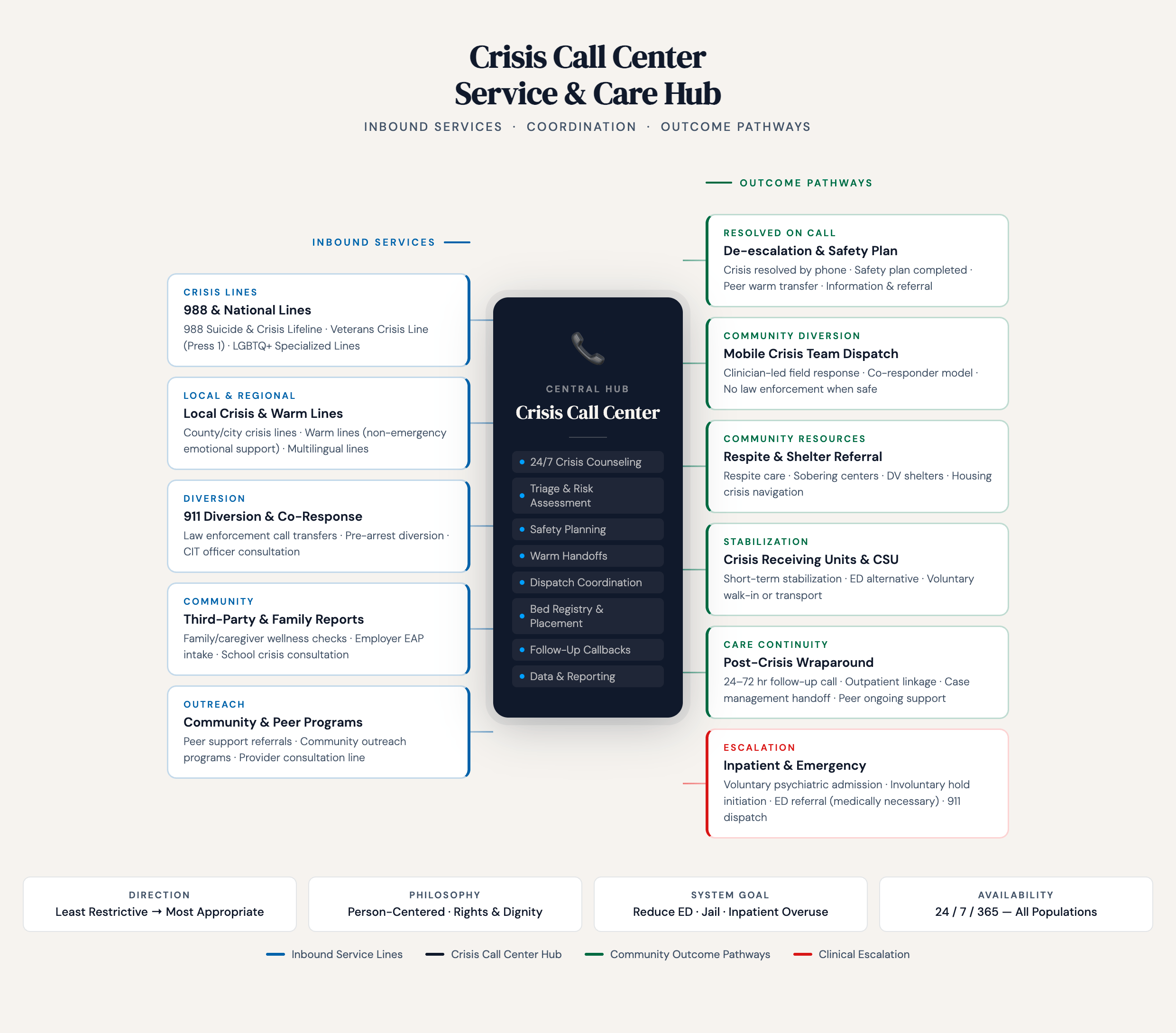
The diagram shows a crisis call center service and care hub. It is organized from left to right, with inbound services on the left, a central crisis call center in the middle, and outcome pathways on the right.
At the top are the labels “Inbound Services,” “Coordination,” and “Outcome Pathways.”
On the left side are five categories of inbound services.
The first category is “Crisis Lines.” This includes 988 and National Lines, such as the 988 Suicide and Crisis Lifeline, Veterans Crisis Line, Press 1, and LGBTQ+ specialized lines.
The second category is “Local and Regional.” This includes local crisis and warm lines, county or city crisis lines, non-emergency emotional support lines, and multilingual lines.
The third category is “Diversion.” This includes 911 diversion and co-response, law enforcement call transfers, pre-arrest diversion, and consultation with crisis intervention team officers.
The fourth category is “Community.” This includes third-party and family reports, family or caregiver wellness checks, employer assistance program intake, and school crisis consultation.
The fifth category is “Outreach.” This includes community and peer programs, peer support referrals, community outreach programs, and provider consultation lines.
In the center is the “Central Hub” or “Crisis Call Center.” This includes 24/7 crisis counseling, triage and risk assessment, safety planning, warm handoffs, dispatch coordination, bed registry and placement, follow-up callbacks, and data and reporting.
On the right side are outcome pathways.
The first pathway is “Resolved on Call.” This includes de-escalation and safety planning, with crisis resolved by phone, safety plan completed, peer warm transfer, and referral information.
The second pathway is “Community Diversion.” This includes mobile crisis team dispatch, clinician-led field response, co-responder models, and situations where law enforcement is not used when safe.
The third pathway is “Community Resources.” This includes respite care, sobering centers, domestic violence shelters, housing services, and crisis navigation.
The fourth pathway is “Stabilization.” This includes crisis receiving units and crisis stabilization units, short-term stabilization, emergency department alternatives, and voluntary walk-in or transport.
The fifth pathway is “Care Continuity.” This includes post-crisis wraparound, 24-to-72-hour follow-up calls, outpatient linkage, case management handoff, and ongoing peer support.
The sixth pathway is “Escalation.” This includes inpatient and emergency care, voluntary psychiatric admission, involuntary hold initiation, emergency department referral when medically necessary, and 911 dispatch.
At the bottom are four guiding principles.
The first is “Direction,” described as moving from least restrictive to most appropriate.
The second is “Philosophy,” described as person-centered, rights-based, and focused on dignity.
The third is “System Goal,” described as reducing emergency department, jail, and inpatient overuse.
The fourth is “Availability,” described as twenty-four hours a day, seven days a week, for all populations.
A legend at the bottom shows color coding for inbound service lines, the crisis call center hub, community outcome pathways, and clinical escalation.